
A federal court recently dismissed a legal challenge (PDF) to the Johnson Amendment on procedural grounds, leaving the door open for current and future appeals. Public discourse surrounding the amendment has focused largely on the legal and political dimensions (PDF), but the public health implications have received much less attention.
The Johnson Amendment is a provision of the tax code enacted in 1954 that prohibits 501(c)(3) organizations such as churches and charities from participating or intervening in any political campaign on behalf of a candidate. Currently, nonprofit organizations, including religious institutions, can discuss issues broadly (PDF), but repealing this amendment could enable institutions to exert greater, more direct influence in political campaigns for office, including by endorsing or opposing political candidates.
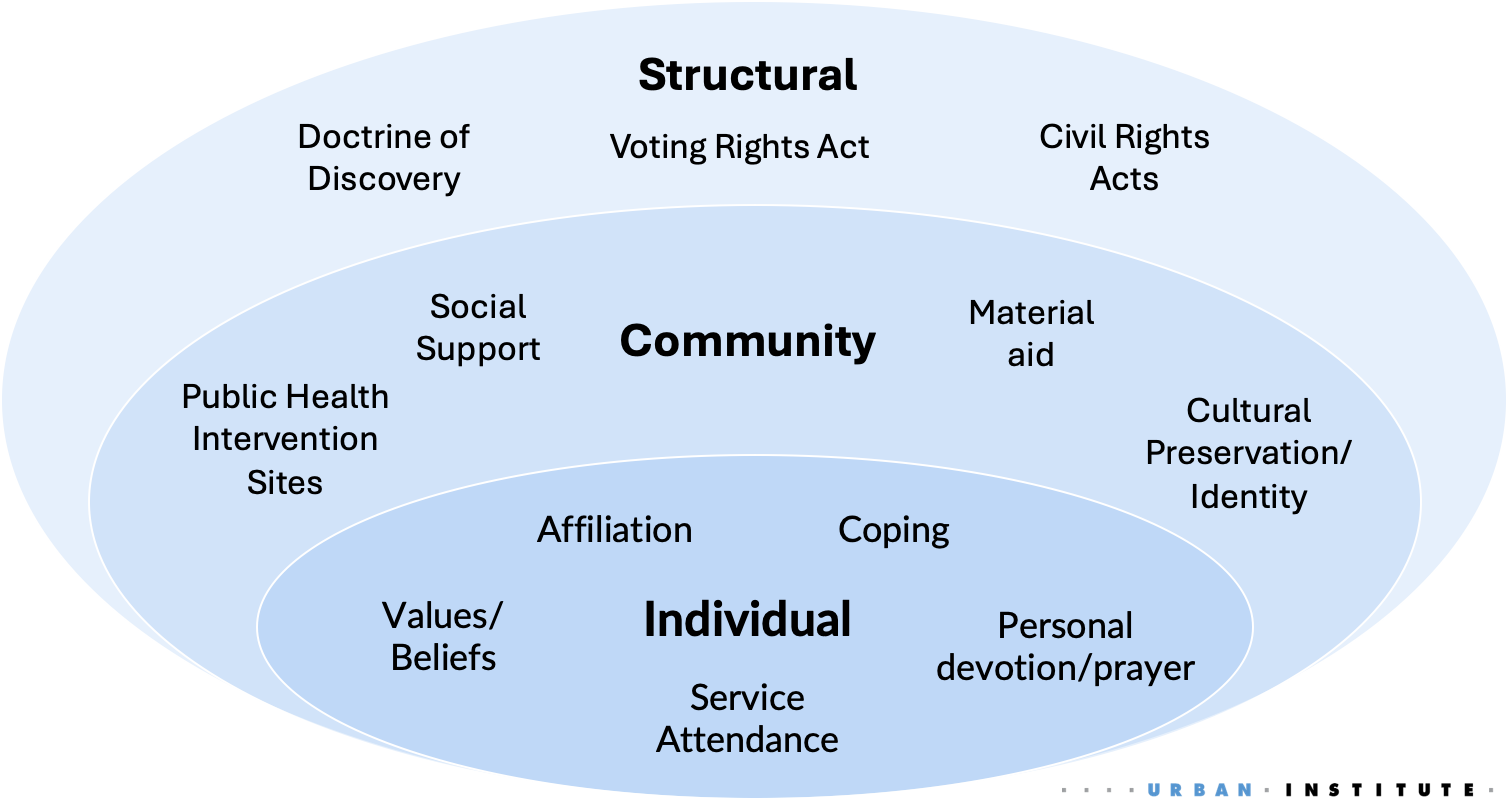
The fate of this amendment matters for population health because religious institutions aren’t only places of worship—they’re also trusted community anchors with broad social influence. A robust body of public health scholarship establishes that religion operates as a multilevel determinant of health that shapes outcomes through individual behavior, community infrastructure, and structural factors. Expanding the political role of religious institutions could therefore reshape not just civic life but also the systems that influence health.
At this moment, policymakers need to understand the link between faith-based values and health infrastructure, and faith leaders need to strengthen their policy literacy. This creates an opportunity for public health scholars to bridge the gap and build the evidence base.
Religiosity and individual behaviors
Research has found higher rates of religious service attendance to be associated with longer life expectancy, better mental health outcomes, and lower rates of cardiovascular disease (PDF). These associations operate through several pathways. For example, religious engagement can serve as a stress buffer, helping people cope with adverse experiences and find purpose in life. Additionally, worship service attendance is linked to health-protective behaviors such as reduced smoking and lower alcohol consumption (PDF).
Community infrastructure
Beyond individual practices, the social and physical infrastructures of religious institutions are central components of community life. Faith leaders are typically effective communicators who often have strong ties with the public and are viewed as sources of moral guidance. The public health field has elevated the importance of faith leaders as trusted messengers of public health information, especially for communities who have been historically mistreated by the health care system.
Religious institutions also provide spaces for social connection. Congregations can buffer against loneliness, a social determinant of health that the World Health Organization declared an epidemic and a “pressing health threat.”
Religious buildings are also community-embedded physical infrastructure, often providing material goods and venues for public health interventions. For example, a study of 3,777 food pantries (PDF) across 12 US states found that 63 percent were faith based. Religious buildings are also commonly used as locations for distributing health resources by offering nutrition demonstrations, clothing drives, and vaccine drives for the public because of their accessibility in local communities.
Religion and public policy
Perhaps the most consequential but least examined level in public health literature is the pathway from religion to health through policies that structure society. People who attend religious services are more likely to vote (PDF) than those who do not, but the relationship between religious values and policy preferences among religious voters can vary.
Core values shared by many faith traditions, such as caring for the poor, welcoming strangers, and protecting the vulnerable, map directly onto policies that shape access to health care, stable housing, food, and a safe environment. In some cases, religious values can influence support for perceived moral and economic policies. On the other hand, some research supports a competing pathways mechanism, where religiosity is associated with lower support for government social insurance.
In both directions, religious values communicated in places of worship can shape voter preferences on policies that function as upstream social determinants of health, including Medicaid, the Supplemental Nutrition Assistance Program (SNAP), housing programs, immigration policy, reproductive rights, environmental protection, and elder care.
This is where the Johnson Amendment becomes a public health issue. Religious institutions and faith leaders have long been involved in advocacy work—including developing interfaith statements, educating their local community, and meeting with legislators to support policies that align with their values—but the line has been in endorsing specific candidates. If houses of worship gain expanded latitude to directly endorse political candidates or intervene in their campaigns, their influence over health policy will increase. Historically, religious institutions have been forces both for systemic oppression (such as the theological justifications offered for the slavery of Africans and the forced assimilation of Indigenous people) and for transformative social justice (the civil rights movement drew its strategic and moral framework substantially from Black churches). Which direction that influence runs depends heavily on which values religious leaders choose to elevate.
Public health researchers can bridge gaps for policymakers and faith leaders
The Johnson Amendment debate will likely continue, but framing it solely as a First Amendment or campaign finance question misses the inevitable public health implications. The values that religious institutions elevate in policy conversations can have downstream effects on society’s access to health resources.
For the sake of population health, policymakers, religious leaders, public health researchers, and health equity advocates cannot afford to ignore the implications of the status of this amendment. Here are some actions each group can take:
- Policymakers: Policymakers should explicitly account for how faith-based values shape constituent support for health-promoting programs. Framing safety net programs such as Medicaid, SNAP, Social Security around broadly shared religious values such as care for the elderly, the sick, and the poor may be more effective than purely economic or utilitarian arguments. This is not a call to conflate church and state, but a recognition that values-based framing is a legitimate and evidence-supported communication strategy.
Policymakers should also treat faith-based infrastructure as health infrastructure. Faith-based food pantries, vaccine sites, and mental health programs are part of the public health system whether or not they are formally recognized as such. Formalizing these partnerships—with appropriate accountability and resources—can both strengthen access and build trust. - Faith leaders: Religious leaders occupy a unique position: They are both interpreters of sacred traditions and influential shapers of public opinion. This positioning in society benefits from genuine policy literacy, including understanding how decisions about Medicaid reimbursement rates, zoning laws, food assistance eligibility, and environmental regulation affect the people they serve and the ability to clarify when policy and political narratives do or do not accurately describe the tenets of their faith.
- Researchers: Public health scholars have a great opportunity to leverage varied research methodologies, including quantitative, qualitative, data science, and community-based participatory research approaches, to provide evidence on the link between religious values and social safety net policies. This could include conducting spatial analyses of geographic areas of greatest need (e.g., higher rates of food insecurity), using text mining to identify overlap between key passages of sacred texts and policy documents, and conducting data walks to elevate resident-defined needs and policy gaps in local communities.
Let’s help communities build more secure, hopeful futures.
Today’s complex challenges demand smarter solutions. Urban brings decades of expertise to understanding the forces shaping people’s lives and the systems that support them. With rigorous analysis and hands-on guidance, we help leaders across the country design, test, and scale solutions that build pathways for greater opportunity.
Your support makes this possible.